
Although small, dental wedges play an irreplaceable role in restorative dentistry. They are mainly used for tooth separation, stabilizing matrix bands and shaping the edges of restorations. Depending on the material and design, the clinical performance and use of wedges vary. In this article, we will systematically analyze the types of dental wedges, their material properties, their main functions and their application in filling and restoration.
1. Types of Dental Wedges and Material Properties
Plastic Dental Wedges
Material: often made of medical polypropylene (PP), flexible.
Advantages:
- Moderate elasticity reduces pressure on gums.
- Can be sterilized at high temperatures and is suitable for reuse.
Disadvantages:
- Limited support, not suitable for cases with deep caries or tight gaps.
Sample Display:
- dental wedges guards (GD-5675): with hole with rblade
three size: Large/Medium/Small

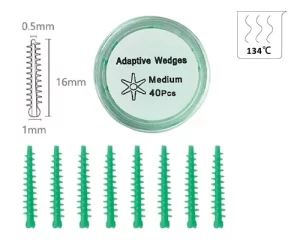
- adaptive wedges (GD-5677): with firm inner plastic core, covered with silicone
- resin dental wedges (GD-5678): four size, XS/S/M/L
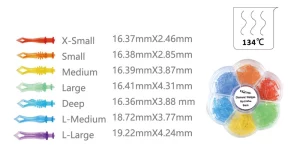
- diamond wedges (GD-5679): seven size, X-small/Small/Medium/Large/Deep/L-medium/L-large

- Tulwar wedges (GD-5680): three size, Small/Medium/Large



Wooden Dental Wedges
Material: mostly birch or pine, sterilized. Birch wedges with a water content of 12% can expand by up to 18.7% in 30 minutes in a gingival fluid environment. This adaptive property makes them particularly suitable for cases of gingival recession in old patients. However, care should be taken: over-expansion may lead to excessive pressure on the periodontal membrane, triggering postoperative sensitivity.
Advantages:
- Naturally water-absorbent and swellable, better fitting to the gap intraoperatively.
- Rigid, suitable for high strength support of Class II cavities.
Disadvantages:
- Non-reusable, over-expansion may cause discomfort.
Samples Display:

Other Types
- Metal Wedge: Rare, commonly used for full crown preparation or special restorative scenarios.
- Silicone wedge: soft and flexible, suitable for aesthetic restorations, but more costly.
2. The Three Core Functions of the Tooth Wedge
Tooth Separation
- Temporarily separates neighboring teeth by 0.2-0.5 mm with light mechanical force to create an operating space.
- This prevents the restoration from overhanging and restores the natural shape of the neighboring points.
- Clinical studies have shown that the proper use of wedges can reduce the risk of food impaction by up to 60%.
Matrix Band Stabilization
- Dental wedges can assist in fixing the molding piece, preventing leakage of the restorative material and shaping the ideal contour.
- Cavity II restorations: the combination with the Matrix Bands stabilization is the classic solution.
- Cavity Class V restorations: usually in combination with a curved molding plate.
Gum protection and hemostasis
- Dental wedges can provide a certain degree of protection above the gums.
- After the dental wedge is inserted into the tooth, it will exert a slight pressure on the gum, reducing bleeding during the operation.
3. Application Skills in Filling and Repair
How to choose the right wedge
| Criteria | Recommended Wedge Type |
|---|---|
| Narrow interproximal space | Wooden wedges, it’s expand and fit together after getting wet |
| Wide interproximal space | Plastic wedge, elastic fit |
| Light-cured resin | Clear plastic wedges, facilitate light penetration |
| Amalgam filling | Wooden wedges, it can offer stronger support |
Insert the Angle and direction
The dental wedge should be inserted obliquely into the interdental space from the lingual or buccal side of the tooth, and the Angle should be controlled at 30° to 45°. The core purpose of this Angle design is to avoid the gum tissue, prevent direct compression or scratching of the gum during vertical insertion, and reduce the risk of postoperative gum redness, swelling and bleeding.
Insertion depth control
The top of the wedge should be slightly higher than the edge of the restoration by approximately 0.5mm. This reserved space is designed to compensate for the shrinkage during the curing process of subsequent filling materials (such as resin), ensuring that the material can closely adhere to the edge of the tooth after curing and avoiding the formation of gaps that could lead to secondary caries.
Clinical precautions
Avoid excessive pressure on the gums: During the operation, the insertion force of the dental wedge should be controlled. Excessive pressure can damage the attachment relationship between the gums and the teeth, which may cause postoperative gum recession. Clinical statistics show that the incidence of such complications is approximately 3% to 7%.
Precise positioning of the insertion position: If the dental wedge is inserted at an offset position (such as being too close to the occlusal surface or the root tip direction), it may cause the contact points of adjacent teeth to be too loose, thereby affecting the stability of the normal occlusal relationship. Patients may experience problems such as weak bite and food impaction.
Actual case: Repair of deep wedge-shaped defect
Taking the repair of a deep wedge-shaped defect of the left lower first premolar as an example, the specific operation and therapeutic effect are as follows:
- Preoperative assessment: The patient was a 45-year-old adult. The cervical defect of the left lower first premolar had reached the deep dentin, accompanied by obvious cold and heat sensitivity symptoms. The Visual Analogue Scale (VAS) was used to assess the sensitivity degree, with a score of 6/10.
- Key operation techniques: First, use the No. 00 gingival line for gingival drainage treatment. Then, insert a pre-moistened pine wedge and let it stand for 15 minutes until it fully expands to widen the tooth gap. Next, fluid resin is used as the base, and then 3M Z350XT resin is used for layered filling. The wedges should be retained until the resin has initially cured before being removed to prevent material deformation during the filling process.
- Postoperative efficacy: The patient was followed up for one year after the operation. The examination showed that the integrity rate of the restoration reached 98%, with no loosening, detachment or secondary caries. The patient’s cold and heat sensitivity symptoms completely disappeared, and the occlusal function returned to normal.
4. Purchasing Criteria for Dental Wedges
Material Safety Priority
Core certification standards
The material and sterilization treatment of the wedge must comply with professional medical standards. Different materials correspond to clear certification requirements:
- Plastic wedges: Must have FDA (Food and Drug Administration of the United States) or CE (European Union Product Safety Certification) medical-grade polymer certification. The core needs to avoid harmful substances such as phthalates, which may migrate through contact and pose potential health risks. Compliance certification is the key basis for ensuring the safety of materials.
- Wooden wedges: A complete EO (ethylene oxide) sterilization report must be provided, and the report should clearly state that the biological load is ≤10⁻⁶ (i.e., the probability of microbial survival after sterilization does not exceed one in a million), ensuring that there are no pathogenic bacteria remaining before use to avoid cross-infection or postoperative inflammation.
Key points to avoid pitfalls in procurement
When purchasing, be cautious of non-medical grade products and especially reject “industrial wooden wedges” without any marking. Most of these products are made from leftover materials from industrial processing and have not undergone medical-grade treatment. They may contain harmful chemicals such as formaldehyde. When used, they not only easily irritate the gum tissue but may also be absorbed through the oral mucosa, posing a threat to the patient’s health. Moreover, there are no unified standards for their size and hardness, which cannot meet the precise operation requirements of dental restoration.
Maximize the size fit rate
When choosing wedges, it is necessary to combine the actual clinical needs and maximize the size fit rate through “preoperative assessment + multi-specification reserve”.
Before the operation, the size of the required wedge should be initially determined based on the width of the interdental gap of the affected tooth (such as the interdental caries gap, wedge-shaped defect gap) and the tooth morphology (such as deciduous teeth and permanent teeth, normal teeth and inclined teeth).
It is recommended to stock up on multiple sizes of wedges (such as thin, medium, thick, or thin and thick styles for special tooth gaps) to avoid poor fit due to insufficient single size, which may affect the gap opening effect or cause gum compression. This ensures that a matching model can be found for different cases, improving operational efficiency and restoration quality.
5. Conclusion
Although dental wedges are small in size and seem insignificant, they are indispensable “key supporting roles” in dental restoration operations. From material selection to standardized use, precise control over every link is not only the core guarantee for enhancing the stability of the restoration and reducing postoperative complications, but also can effectively improve the patient’s diagnosis and treatment experience and lay a foundation for a long-term good prognosis.
